Choosing an ACL Graft – what is your best option?
If you’ve torn your ACL and you are debating surgery, deciding on the type of graft to use to reconstruct the ligament can be a source of significant anxiety and confusion. You may encounter conflicting information on the chance of suffering a re-rupture based on the graft source, as well as the potential downsides of a particular graft. In this article, we will discuss the options, and I will outline the factors that I discuss with my patients to help them choose the best graft for their lifestyle and activity level.
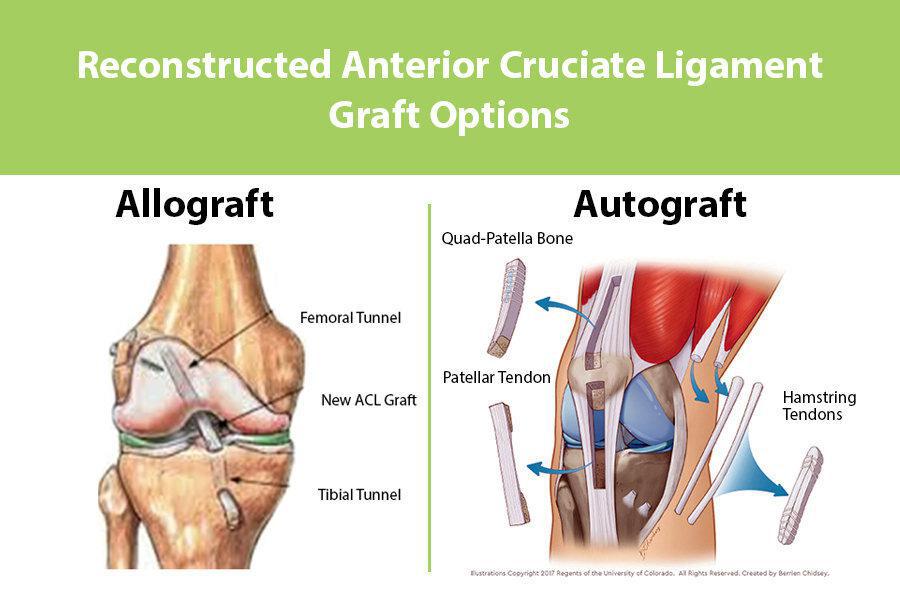
Autograft vs. Allograft
ACL grafts are broadly characterized in to autografts and allografts. Autograft tissue is obtained from another part of the patient’s own body, while allografts are obtained from a tissue donor. Autograft tissue generally is harvested from around the injured knee. In rare cases, autograft tissue may be taken from the patient’s non-injured knee.
The advantages of autograft tissue are the following:
- Autograft tissue has a lower re-rupture rate in younger, high-activity patients
- Your body will not reject autograft tissue
- No risk of disease transmission
- Faster incorporation/return to full activities
- Lower cost
The disadvantages of autograft tissue include:
- Greater post-operative pain
- Potential for knee pain or weakness
- Potential for a second scar over the area where the tissue is harvested
The advantages of allograft include:
- Less post-operative pain
- Smaller scars
- Easier rehabilitation
- No graft harvest site issues
The disadvantages of allograft include:
- A higher re-rupture rate, particularly in young, active patients
- A small risk of disease transmission or graft rejection
- Higher cost
Generally speaking, I prefer autograft tissue over allograft tissue in most patients. It is more reliable, and ultimately, give me the confidence to allow the patient to return to their sport sooner.
There are three common sources for autograft ACL:
- Patella Tendon
- Hamstring Tendon
- Quadriceps Tendon
In the young, high-level, or profession athlete, I will almost exclusively use patellar tendon autograft. This is the “gold standard” for ACL reconstruction with the longest track record of success. Overall, it has the lowest re-rupture rate and lowest likelihood of stretching out over time. The downside of this graft is that it is harvested from the front of the knee and can be associated with post-operative pain in certain patients. This is usually due to poor rehab, and consequently, can be avoided in most cases with appropriate physical therapy and strenghtening of the muscles around the knee.
For patients who would like to avoid the possibility of anterior (front) knee pain, or already have a history of anterior knee pain, I would advise the use of a hamstring tendon graft or quadriceps tendon graft. Both of these are excellent alternatives to the patella tendon graft.
Hamstrings also have a long track record but do have a small increased risk of stretching out over time, particularly in young females. Quadriceps tendon graft is a relatively new option but the short-term results are promising. It is a large, strong graft, and is well suited for young patients, and it is also very useful in cases of revision (redo) ACL surgery where a hamstring or patellar tendon graft may have already been harvested.
I reserve allograft for patients who are low-demand or those who simply do not want to use their own tissue.
The common sources for allograft tissue include:
- Achilles’ Tendon
- Patella Tendon
- Hamstring Tendon
Each of these have very similar biomechanic and biologic properties. If you choose to use allograft, speak to your doctor about the graft that she or he prefers, and the type of sterilization or processing that is utilized. In general, grafts that are harvested in a sterile fashion and minimally processed have the best biomechanical properties. Consequently, they may have lower re-rupture rates, but this is not definitively supported by the literature.
To summarize, ACL surgery is not a “one size fits all” procedure. The surgeon should work with the patient to determine which approach is best for them, and will yield the lowest risk of re-injury, and the greatest likelihood of return to sport.

